

Abstract
Introduction
Haemophilia A (HA) phenotypes (mild, moderate and severe) are based on the baseline FVIII levels, however considerable variation in the bleeding phenotype exists between patients with similar FVIII level. Moreover, approximately 40% of patients with mild HA have large discrepancies between FVIII measured by one stage (FVIII:C1) and two stage methods (FVIII:Chr2) and it is unclear which method correlates best with in vivo FVIII function and bleeding phenotype. The Thrombin Generation assay (TGA), a global measure of haemostasis may be a better predictor of bleeding phenotype but pre-analytical factors such as contact activation can confound the results. Choice of initiating conditions may also be critical in determining sensitivity: recent studies have suggested that initiation with FIXa rather than tissue factor (TF) in detecting low levels of FVIII:C in severe HA, however its utility in mild to moderate HA patients has yet to be determined.
The aim of this study is to establish the relationship between FVIII:C and TGA and the influence of contact factor activation in TF and FIXa triggered TGA in patients with mild to moderate HA.
Methods
This is a prospective cohort study. Patients aged >18 with known congenital HA and FVIII:C 0.01- 0.2 iu/ml were recruited from 3 Haemophilia Comprehensive Care Centres in London. Peripheral blood was drawn into citrate Vacutainer tubes containing 0.106M trisodium citrate (1:9 volume) and Vacutainer tubes preloaded with CTI (50µg/ml). Samples underwent double centrifugation (2500g) to obtain platelet free plasma. Thrombin generation assay, using a standard calibrated automated thrombogram was triggered with either TF (1pmol) or FIXa (5nM). Factor FVIII levels were assessed by one stage APTT based (FVIII:C1) and two stage chromogenic (FVIII:Chr2) methods. Mutation analysis was carried out in all patients.
Results
40 patients were recruited in the study. Five patients (13%) had standard FVIII discrepancy (FVIII:C1/FVIII:Chr2>1.5) with 4 different FVIII mutations located on the inter-domain surface of the A2 domain (p.Tyr683Ser, p.Arg550Cys, p.Gly498Arg, p.MET681.Le). One patient had reverse FVIII discrepancy.
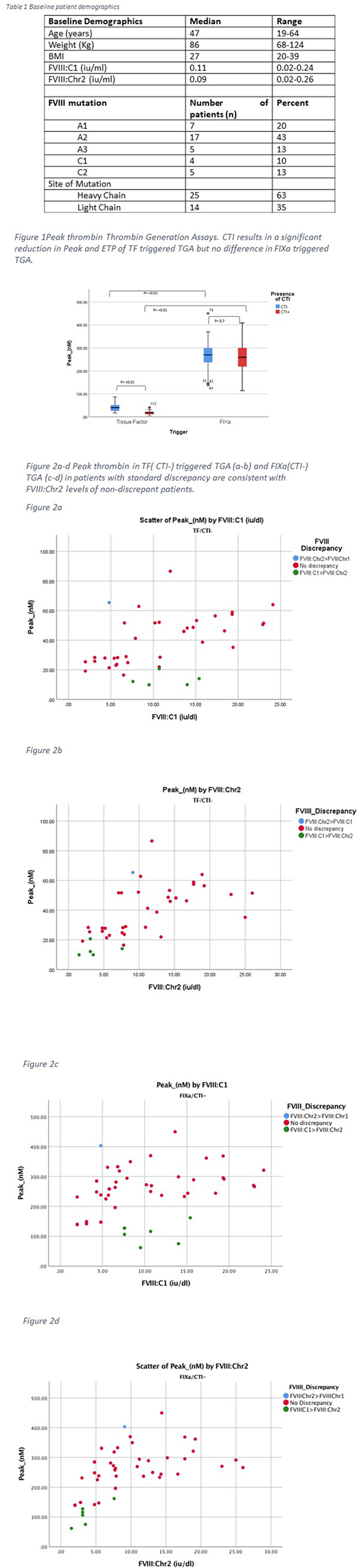
In TF triggered TGA, the presence of CTI resulted in significant reduction in mean ETP (nmol .min)(455. vs 278, p<0.01, 95% CI 104-243), mean Peak thrombin (nM) (37.81 vs 16.54, t(6.6) p<0.01 95%CI 14.7-27.3), and mean Velindex (nM/min) (4.86 vs 1.29 t(7.0), p<0.01, 95% CI2.3-4.19) and a longer mean ttPeak (min) (14.26 vs 16.22, t(-3.2) p=0.02 95% CI-3.1- -0.76). In contrast, the presence of CTI did not affect ETP (1143 vs 1042, p=0.19 95% CI -54-256), mean Peak thrombin (252 vs 251, p=0.6 95%CI 27-46) or Velindex (118.54 vs 119.15 p= 0.95, 95%CI -23-12.9) in FIXa triggered TGA.
There was a good correlation between FVIII:Chr2 and ETP (r=0.56, p=<0.001) Peak (r=0.6, p=<0.001) and Velindex (r=0.7, p=<0.001) in TF(CTI-) triggered TGA, however no relationship was seen between FVIII:C and TG parameters (ETP r=-0.01 p=0.9, Peak r=-0.003, p=0.97 and Velindex r=0.018, p=0.9) in TF(CTI+) triggered TGA. In both FIXa(CTI-) and FIXa (CTI+) triggered TGA, there was a good correlation seen between Lagtime (r=-0.6 p=<0.01), Peak (r=0.4-0.6, p=<0.01) ttpeak (r= -0.6, p=<0.01) and Velindex (r=0.69 <0.01) with FVIII:Chr2 but not with ETP.
In patients with standard FVIII discrepancy (n=5), their ETP and Peak levels in TF and FIXa triggered TGA were in keeping with the ETP and Peak levels of non-discrepant patients with similar FVIII:C2 and significantly lower than that of non-discrepant patients with similar FVIII:C1.
Conclusions
Our study confirms that at low TF triggered TG, contact factor activation in vitro is an important preanalytical variable. Curiously any TG correlation with FVIII level is lost once the contact pathway is inhibited suggesting that TG remains largely determined by the extrinsic pathway in this system. In contrast, factor FIXa triggered TG is unaffected by inhibition of contact activation and demonstrates a good correlation to FVIII:C with or without CTI. This can be explained by suggesting that the supply of FIXa negates any effect of XIa from contact activation and that TG by this route is more completely dependent on FVIII. Therefore a FIXa triggered TGA may offer a better alternative in the assessment of haemophilia and further studies are underway to determine whether this is a better predictor of bleeding phenotypes.
Luo:Pfizer: Research Funding. Austin:Pfizer: Research Funding. Laffan:Pfizer: Honoraria; Roche: Consultancy, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal